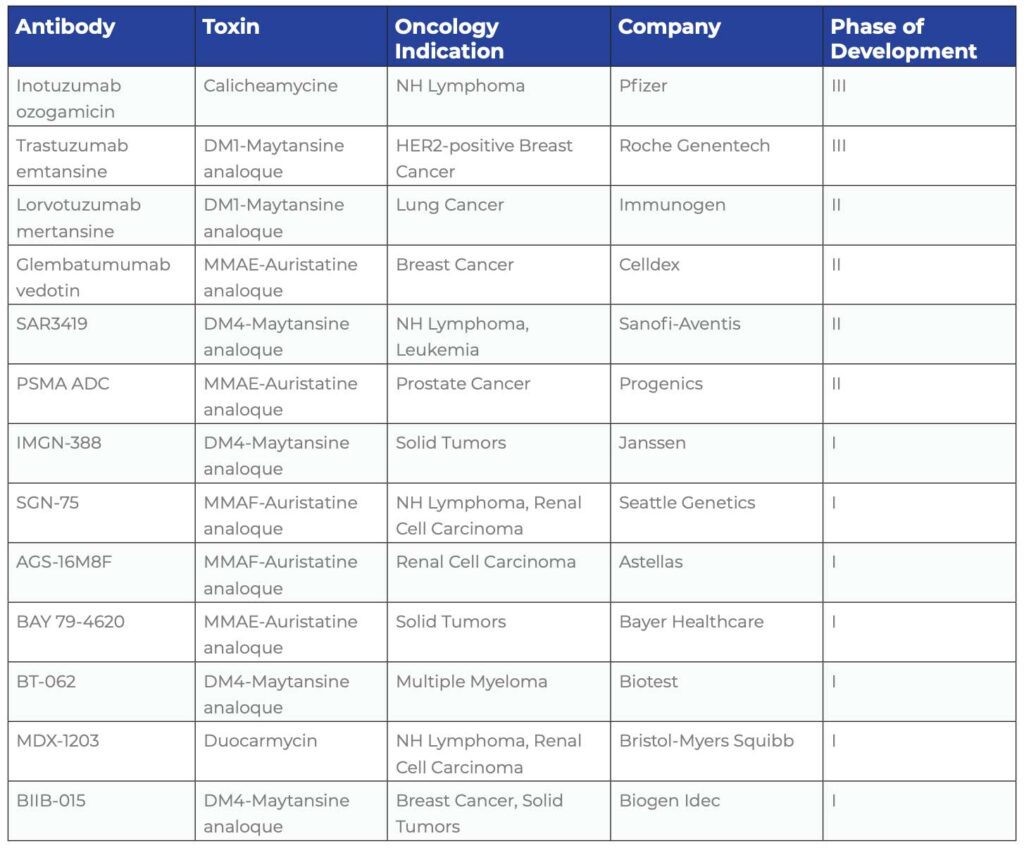
These recent advancements in linker chemistries have led a lot of biotech companies to take another look at their portfolios of “naked” antibodies. Antibodies that have failed in Phase I or II are being scrutinized again. In addition to novel antibodies, already approved antibodies are also being used as bases for ADCs. After positive Phase II studies, Genentech is now conducting Phase III studies for an ADC of trastuzumab linked to the cytotoxic agent, emtansine in patients with HER2-positive breast cancer. The company has recently filed a Biologics License Application (BLA) with the US FDA.
The advantage of using a therapeutically proven antibody agent such as trastuzumab is that there is already a lot known about the antibody itself as well as its pharmacological target, which in this case is the tumor cell membrane protein HER2.
The efficacy of an ADC is largely dependent upon how many copies of the target are expressed on the tumor cells and how fast the ADC is being transported into the tumor cell. In general, rather high copy numbers (> 100,000 per cell) are required to import enough toxin to kill the cell. Despite advances in ADC engineering, only a fraction of the total injected antibody dose can be effectively delivered to the target tumor. Hence the cytotoxic agent bound to the antibody needs to be highly potent so that any ADCs that do reach their target cells have the maximum killing potential.
This highly complex balancing act is typical for the development of ADCs, which not only requires the merging of biotechnology and organic chemistry derived technologies but also requires a thorough understanding of the biological complexity of the targets as well as the handling of extremely potent toxins. Nonetheless, future prospects for ADCs seem to be bright even though it has been hard to predict how certain tumor types will actually respond to treatment. Only clinical trials can predict how well this promise will pay off to benefit patients.